| Origination | 6/27/2017 |
|---|---|
| Last Approved | 5/18/2026 |
| Effective | 5/18/2026 |
| Last Revised | 5/18/2026 |
| Next Review | 10/11/2026 |
| Owner | Quinlan, Amy |
|---|---|
| Policy Area | URM Cardiac Care - VAD |
| Applicability | University of Rochester - Strong Memorial Hospital |
| Reference | URM Cardiac Care |
search terms: VAD, LVAD, blood pressure, hypertension, hypotension, doppler, MAP
Objective Copy Link
Establish a set of guidelines to direct blood pressure management for LVAD patients.
Background
The goal of LVAD therapy is to utilize the pump to unload the left ventricle by setting the speed to provide a pulse pressure of 10-20mmHg. Pharmaceutical therapy is used to maintain a goal mean arterial pressure (MAP), which optimizes pump flow, often resulting in an absence of a radial pulse. There are multiple factors that affect speed settings and blood pressure targets in LVAD patients.
Measuring Blood Pressure
- For patients with an arterial line, a Doppler pressure should be assessed prior to arterial line removal with both values documented. This allows comparison between Doppler pressure and arterial line pressure.
- Treatment of blood pressure is based on the MAP regardless of the method used.
- How to obtain a doppler blood pressure:

- Doppler is considered the standard method to obtain blood pressure unless a
strong radial pulse is palpable. See graphic below: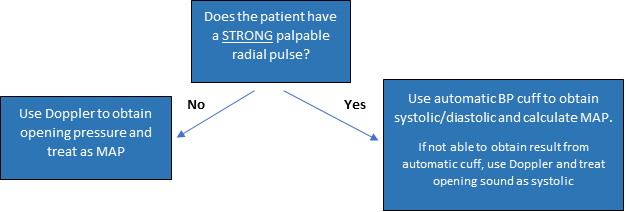
- Inpatient providers, working with the nursing staff, will determine the best method to measure BP.
- Providers should be made aware when a patient is newly pulsatile as this may necessitate further evaluation.
Target Blood Pressure
- Acceptable MAP 75-90mmHg
- Ideal MAP 80-90mmHg
- MAP goals will be adjusted on an individual basis as necessitated by clinical situation
Low Blood Pressure Management in the Hospital Setting
- MAP 60-75mmHG:
- MAP<75 may be permissible in some patients if there is adequate end organ perfusion (UOP>50 cc/hr, normal mentation, normal lactate)
- Consider holding/adjusting outpatient anti-hypertensive medications
- Consider small (250-500mL) IV fluid bolus if pt felt to be dehydrated. **use caution in patients with poor right ventricular function**
- In the ICU and immediate post-VAD implant patients: do not initiate or titrate vasopressors for MAP 60-75mmHG, unless the primary attending is aware
- MAP less than 60mmHg:
- Consult the LVAD attending/APP and address underlying causes.
High Blood Pressure Management
- Defined as MAP >95mmHg.
- Adjustments to antihypertensives will be directed by Advanced Heart Failure Clinician.
- Preference should be given to medications patients have already been approved for and tolerated in the past unless the current clinical situation dictates otherwise.
- Use a tier system working first from Tier I down to Tier III. Multiple medications within a tier may be used at moderate doses to avoid adverse effects from high doses.
- Clinical condition will dictate changes to regimen.
- LVAD patients awaiting transplant will be transitioned to short acting agents as determined by transplant coordinator.
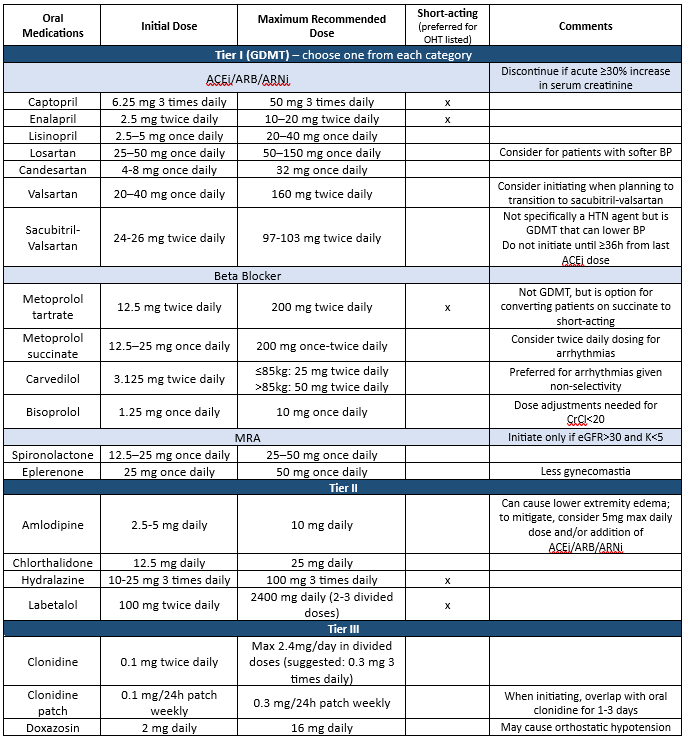
Abbreviations: ACEi (angiotensin-converting enzyme inhibitors), ARNi (angiotensin receptor-neprilysin inhibitors), ARB (angiotensin (II) receptor blockers), BP (blood pressure), CrCl (creatinine clearance), eGFR (estimated glomerular filtration rate), GDMT (guideline-directed medical therapy), HTN (hypertension), MRA (mineralocorticoid receptor antagonist), OHT (orthotopic heart transplant), SGLT2i (sodium-glucose cotransporter-2 inhibitors), T2DM (type 2 diabetes mellitus)
ICU or ED
- Hydralazine (PO/IV) until stable and then give Tier I or II (if clinically appropriate) or prior outpatient oral medications
- Nicardipine infusion: initiate infusion at 5mg/hr, may titrate to a maximum of 15mg/hr. Once BP controlled, decrease rate to 3mg/hr and titrate as needed to response.
- Labetalol IV: initial dose 10-20 mg Q10min, may increase up to 80mg. Max total cumulative dose 300mg.
PRN Use
- Hydralazine 25mg PO Q6hr PRN MAP ≥ 95
- Recheck MAP 1-2 hours after prn given
- Call covering provider if MAP remains above goal after prn x 2 given
- **Preference is to adjust daily antihypertensive medications instead of administering prn medications. RN should contact covering provider during daytime shifts prior to giving prn medication**
Permissive Hypertension Guidance
Refer to the following UR guideline for suspected acute ischemic stroke: UR Medicine Cardiac Care - VAD Stroke Management Guideline